
Turning the Ship Around is Possible
VHC911 – Stat v.23
The Cost and Quality Challenge at UVMMC: Turning the Ship Around is Possible
There is broad agreement that healthcare costs in Vermont are too high. State leaders, hospital executives, insurance CEOs, state regulators, business and union leaders and the public all agree we are in a crisis.
First, let’s agree on an affordability metric
Reducing costs in healthcare requires metrics. Without a common yardstick, we are left with competing narratives that can cloud the horizon. At the pump we all have faith that a gallon is a gallon. In healthcare we don’t have similar standards for the public and policy leaders to use. Healthcare spending is so complex and operates in its own world.
This complexity has become a shield that blocks public accountability and scrutiny. In Vermont, we have seen steady growth to the point that healthcare spending now approaches 20% of the state’s GDP. And, as we’ve discussed, in the last few years hospital spending is the fastest growing segment of healthcare spending.
To know if we are truly making progress in lowering excessive hospital prices, we should use Medicare as the primary benchmark.
Medicare as a Yardstick
Medicare is the largest public payer in the nation and in Vermont (23% of Vermonters are covered by Medicare). Medicare hospital prices are set administratively by the federal government using a “Prospective Payment System” (PPS) for larger hospitals and a cost per service model for small, critical access hospitals. Both of these establish predetermined, fixed rates for services. These rates can be considered the actual cost of a procedure at any hospital in the country. T
he Medicare rate-setting system is consistently administered from state to state. The rates are constructed to cover operating costs (labor, supplies), capital-related costs (depreciation, property-related insurance and taxes), and market conditions in the hospital’s location (such as labor costs through a wage index). They are also adjusted to reflect a patient’s clinical condition and related treatment costs. This rate setting process is updated annually through federal regulations to account for inflation and productivity.
In short, Medicare works hard to get this right. The rate-setting process and updates are largely predictable for hospitals and health care providers. This makes Medicare rates as good a metric as we have in the US to answer the straightforward question: how much does “X procedure” cost?
A Tale of Two Academic Medical Centers
University of Vermont Medical Center & University Hospitals Cleveland Medical Center
Once we understand that Medicare is a useful benchmark to explain costs, then measuring a hospital’s profit/loss when treating Medicare patients starts to make sense. It’s not really about the money made or lost treating seniors – it’s simply a shortcut to look at overall efficiency. If a hospital can meet its costs from Medicare payments, then we know overhead and administrative costs are where they should be.
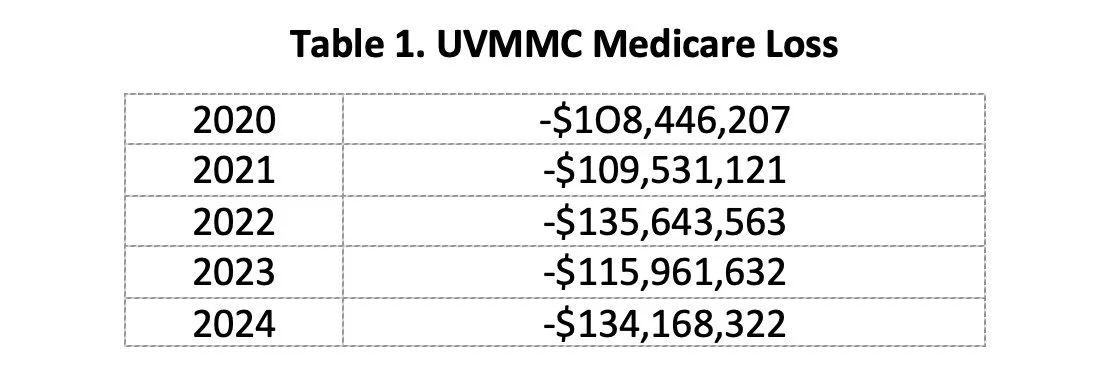
UVMMC has historically performed poorly on this measure since 2020. Table 1 shows that UVMMC has lost over $600M treating Medicare patients between 2020-2024.
When a hospital can’t cover costs for Medicare patients, they turn to commercial insurance to make up the difference. After years of this dynamic, Vermont finds itself with the highest commercial insurance rates in the nation. And unfortunately, declining performance on key quality measures, too.
While UVMMC is among the worst 10% of AMCs for losses to Medicare, it is hardly alone.
University Hospitals Cleveland Medical Center (UHCMC) is a comparable institution. It’s a bit bigger (656 vs. 468 beds), but, like UVMMC, it serves as the anchor facility in its respective health network.
In 2020, the University Hospitals Cleveland Medical Center (UHCMC) lost $27M treating Medicare patients. The next year, when losses grew to $70M, the hospital committed to a new direction. Using a quality and efficiency framework with Medicare as a yardstick, UHCMC reduced its Medicare losses to $20M in 2024. In comparison UVMMC, with one-third fewer beds, lost more than six times as much on Medicare in 2024 (-$134M) as did the Cleveland Medical Center.
To get costs under control requires a leadership and care-delivery transformation framework that drives toward a high-value system: improving access and quality in a cost-effective manner for patients and payers.
After hearing testimony from Dr. Peter Pronovost, Chief Quality and Transformation Officer, at the University Hospitals of Cleveland (UH of Cleveland) health system (Green Mountain Care Board in March 2025, VHC911 began to take a closer look at their efficiency framework. It is focused on improving care and efficiency and not simply cost cutting. It has four broad goals:
Get paid fairly
Improve access
Reduce cost per visit/discharge
Maximize quality performance
Initiated in 2022, the framework is improving quality and access and driving greater operational efficiency, all while measuring how close the UHCMC and its network can come to living within Medicare reimbursements. The framework engages every single employee in identifying and testing improvements and measuring results. It prioritizes direct patient care and requires rigorous accountability and teamwork from staff.
Key approaches include eliminating policies and procedures that do not add value, developing functional organizational charts, and reducing administrative expenses. Additionally, working with on-the-ground staff, hospital leaders identify measurable goals to improve access and reduce costs per discharge, then perform a comprehensive assessment of actual outcomes.
Most impressive is a care culture that values the contribution of each employee, of learning and not fearing, and one in which everyone is heard. The principles are straightforward; the execution is extremely detailed. The results offer a promising roadmap that we believe can work in Vermont.
The UHCMC approach resonates with VHC911 because it suggests a quick turnaround is possible. The framework could help undo the layers and layers of administration and management in the UVM Health organization. It is also an antidote to the consolidation of decision-making at the network level which leaves local teams and hospitals dis-empowered.
Dr. Leffler and his team at UVMMC agree with the goal of “breaking even” on Medicare and have publicly committed to getting there within the next five years. The quality and efficiency framework at UHCMC is impressive and echoes the other commitment Dr. Leffler makes repeatedly: to improving quality across UVM Health.
Both UVMMC and UHCMC Lost Significant Money on Medicare
Since 2020, leaders at Vermont’s Academic Medical Center and UVM Health repeatedly responded to Medicare losses by pushing up profits from commercial insurance payers. Figure 1 looks at the profits/losses per adjusted patient discharge for Medicare and commercial insurance
Figure 1. Comparison of UVMMC and UHCMC profits (losses) per adjusted patient discharge (APD) from Medicare and commercial insurance.
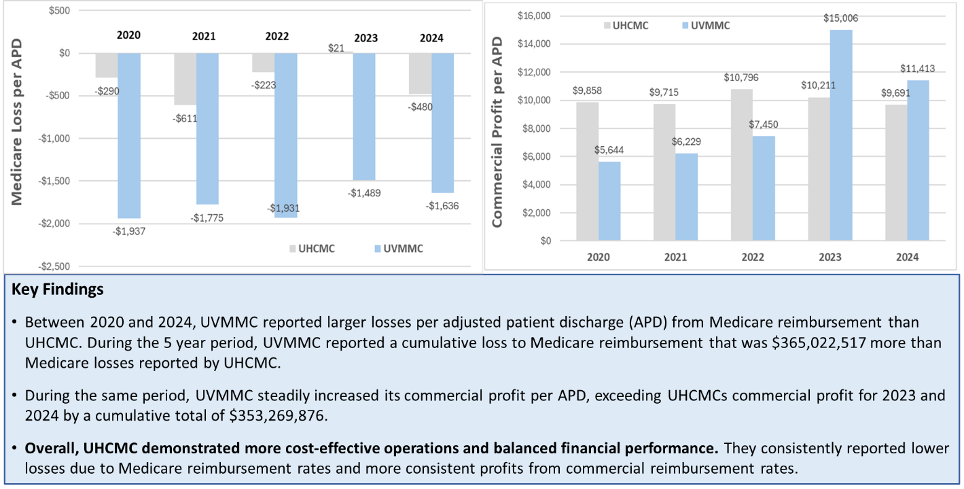
The cumulative losses from Medicare reported by UVMMC during the five-year period were $365,022,517 more than the larger UHCMC. At the same time, in 2023 and 2024, UVMMC accumulated $353,269,876 more in total profits from commercial insurance than did UHCMC. This accumulation of commercial profits is a significant driver in Blue Cross of Vermont’s brush with insolvency.
Comparing Overall Profits
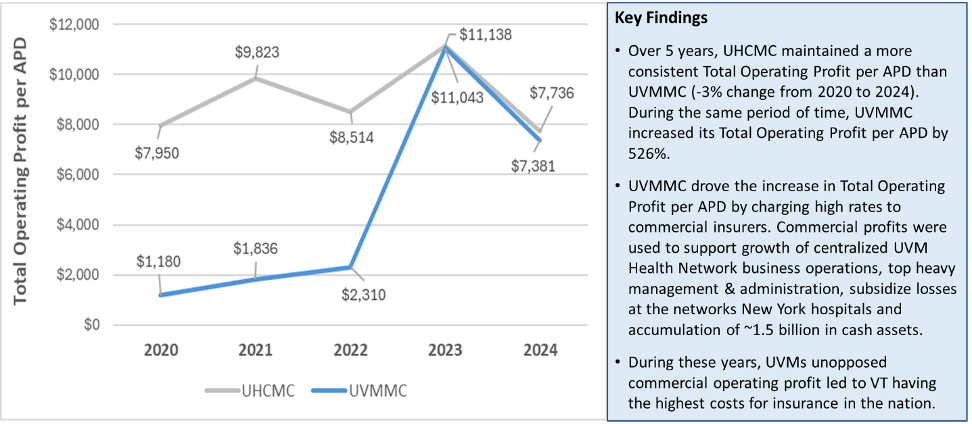
What is evident in Figure 1 is UHCMCs more balanced financial performance from 2020 to 2024, with relatively small losses from Medicare reimbursement and relatively consistent profits from commercial reimbursement. This dynamic is amplified when you look at total operating profits per discharge across the same time span (Figure 2). The pattern is striking in that it shows UVMMC dramatically escalated profits beginning in 2022.
Unfortunately, Vermont’s commercial payors, notably Blue Cross of Vermont, did not challenge the rates and UVMMC’s commercial profits increased by over 500% between 2020 and 2024. The high rates charged to commercial insurers by UVMMC supported the growth of the Health Network’s centralized operations and top-heavy management expenses and subsidized the losses at its New York hospitals. What is also notable is that both organizations had similar operating profits in 2023 and 2024, the difference being that UVMMC had to pull such large profits solely from commercial insurers because of the persistent Medicare deficit. If UVMMCs operated closer to breaking even on Medicare, it would not have had to charge such high rates to insurers such as BCBS of Vermont.
Figure 2. UVMMC and UHCMC total operating profit per adjusted patient discharge.
As shown in Figures 1 & 2, UVMMC could have achieved the same overall profit per discharge in 2023 and 2024 if they operated more cost effectively and come closer to breaking even on Medicare like UHCMC. In essence, UVMMC could have made the profit they needed to operate without driving up commercial rates the way they did in those years.
Profits at the Expense of Patient Care?
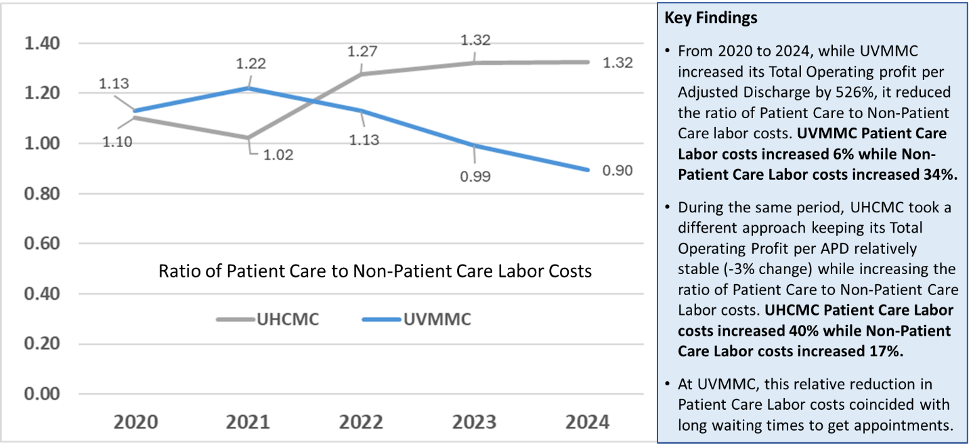
While the profits per adjusted discharge increased 526% at UVMMC, it reduced the ratio of patient care to non-patient care labor costs. Direct patient care labor costs increased 6% over five years, while non-patient care (management and administration) increased by 34%. The relatively low growth in patient care labor costs also coincides with long wait times for clinical care at UVMMC.
The value and efficiency framework implemented at UHCMC shows a very different story. While the UHCMC operating profit per adjusted discharge remained stable (-3%) over the five years, the direct patient care labor costs increased 40% while non-patient care labor costs grew at a slower 17% (Figure 3).
Figure 3. Comparison of UVMMC and UHCMC labor costs for patient care and non-patient care.
Where Do We Go from Here?
To date, Vermont’s reform efforts have failed to contain costs, especially in hospitals. Regulatory approaches aimed at limiting hospital revenue by the Green Mountain Care Board – capitation and risk sharing agreements under the All-Payor Model and ACO and upstream investments in primary care through the Blueprint for Health – have all been insufficient to contain the growth in costs.
This underscores the importance of Act 68 in 2025, which requires the Green Mountain Care Board to implement reference-based pricing for hospital reimbursements across all commercial payers. That appears on track to become a reality in 2028. Managing to Medicare reimbursements offers a clear, measurable goal to drive down operating costs. Reference-based pricing should help translate hospital efficiency to lower commercial charges. That will be essential if we have any hope of seeing lower insurance costs for families, business and taxpayers. Check out our recent webinar that featured leaders in reference-based pricing from Montana and Oregon and explored the potential savings here in Vermont.
VHC911 supports the transformation work necessary for UVMMC to become a high-value medical center and hopes the management framework employed by the UHCMC to “break even on Medicare while improving quality and access” might help achieve this goal.
Dr. Pronovost has been gracious with his time and met with VHC911 board members twice to help us evaluate how such a project could be applied to Vermont and especially at UVMMC and the Health Network. We intend to deepen this collaboration and share what we learn. We urge hospital leaders at UVMMC and the Health Network to do the same.
Vermont Healthcare 911 (VHC911) is a broad coalition united to combat the high cost of healthcare in Vermont. The coalition is composed of business owners, labor leaders, healthcare providers, civic and political leaders of all parties and represents about 200,000 Vermonters.